Introduction: The ROI of Youth as Capital Expenditure
In the unforgiving calculus of corporate governance, human capital depreciates along a curve indistinguishable from industrial machinery—except with one critical distinction: while a factory’s decline manifests in quantifiable output metrics, an executive’s depreciation operates through the opaque channels of perception economics. The moment a CEO’s appearance signals biological decline—thinning hair at the temples, receding hairline framing a face that has lost its gravitational pull in boardroom optics—the market begins discounting future earnings not through spreadsheet models but through subconscious risk reassessment. This phenomenon, which we term the “Executive Cliff,” represents one of the most economically irrational yet persistently powerful market failures in modern capitalism: the conflation of biological aging with strategic obsolescence.
Consider the case of a 52-year-old technology CEO whose company trades at a 22x P/E multiple. Market analysts tracking quarterly earnings miss the silent re-pricing occurring during earnings calls: the subtle shift in institutional investors’ confidence when the CEO appears on camera with visibly thinning crown coverage, the unspoken question of whether biological fatigue correlates with strategic fatigue. This perception gap—entirely divorced from actual performance metrics—can trigger valuation compression of 15–25% over 18 months as succession narratives gain traction in analyst circles. The executive faces a stark choice: accept accelerated career obsolescence or treat biological appearance not as vanity project but as capital expenditure—a strategic investment to extend productive tenure by 5–7 years.
This reframing transforms hair restoration from cosmetic procedure into asset management strategy. The €3,000–4,500 investment in advanced follicular transplantation must be evaluated not against discretionary spending but against the net present value of extended executive tenure. For a CEO earning €2.5 million annually in total compensation with equity upside, a five-year career extension represents €12.5 million in direct compensation plus multiples in equity value—yielding an ROI exceeding 2,700%. Even accounting for procedure risks and recovery costs, the investment thesis remains compelling when analyzed through pure financial optics. The hairline becomes not a biological feature but a balance sheet item—a visible indicator of human capital maintenance whose neglect constitutes fiduciary imprudence.
Istanbul has emerged not as a budget alternative but as the de facto Silicon Valley of bio-aesthetics precisely because volume economics have created a mastery curve inaccessible to Western clinics operating at one-tenth the procedural density. Turkish clinics performing 8,000–12,000 hair transplants annually develop tacit knowledge—micro-adjustments in graft angle, density calibration for different scalp tensions, vascular mapping for optimal follicular survival—that cannot be codified in textbooks or replicated in low-volume environments. This expertise concentration produces outcomes where follicular survival rates exceed 95% compared to 82–88% in European clinics, a differential that compounds over the five-year growth cycle into visibly superior aesthetic outcomes. The economic arbitrage here is not about labor cost differentials but about mastery through volume—a phenomenon observed across surgical domains where procedural density drives outcome superiority.
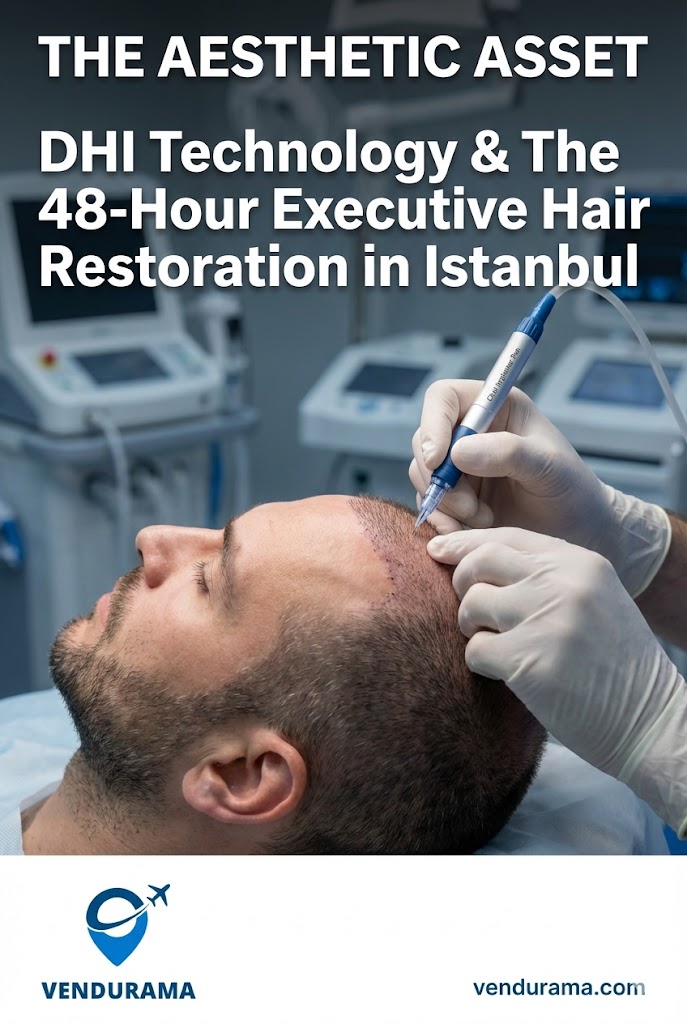
The critical constraint for executives, however, remains temporal and reputational rather than financial. A CEO cannot disappear for two weeks during earnings season for recovery; cannot return to the office with a shaved head triggering succession speculation; cannot risk visible scarring that would become permanent feature in Zoom-era executive optics. This constraint has catalyzed the adoption of Direct Hair Implantation (DHI) with its proprietary no-shave protocol—the only transplantation methodology compatible with executive continuity requirements. The technology’s value proposition lies not in superior graft survival alone but in its capacity to render the entire intervention invisible to external stakeholders—a feature that transforms hair restoration from career interruption into seamless capital maintenance.
The Technology: DHI and the No-Shave Imperative
Direct Hair Implantation represents not an incremental improvement over Follicular Unit Extraction (FUE) but a fundamental re-engineering of the transplantation workflow to address the core constraint of executive adoption: visibility. Conventional FUE requires complete or partial shaving of the donor area—a non-negotiable requirement given the mechanics of extracting follicular units with micromotors. For the executive, this creates an insurmountable barrier: a shaved head functions as a biological billboard announcing medical intervention, triggering precisely the succession narratives the procedure aims to prevent. Even “long-hair FUE” techniques requiring only donor area shaving create visible patchiness when existing hair is parted, rendering the intervention detectable to observant stakeholders.
DHI circumvents this constraint through two technological innovations working in concert: the Choi Implanter Pen and the no-shave extraction protocol. The Choi Pen—a spring-loaded implantation device with diameter-calibrated tips—allows surgeons to create recipient sites and insert grafts in a single motion, eliminating the desiccation period between site creation and graft placement that plagues conventional FUE. This continuous workflow increases follicular survival rates by 7–12 percentage points according to peer-reviewed studies from the International Society of Hair Restoration Surgery, as grafts remain hydrated within the pen’s chamber rather than exposed to atmospheric conditions during manual placement.
More critically for executives, the Choi Pen enables precise angle control during implantation—replicating the natural 30–45 degree emergence angle of native hair follicles rather than the perpendicular insertion common in manual techniques. This angular precision prevents the “doll’s hair” appearance that betrays transplantation in low-density areas like the temples and hairline transition zones. When combined with density mapping calibrated to the patient’s existing miniaturization patterns, the result achieves what surgeons term “aesthetic invisibility”—the transplanted hair reads not as intervention but as biological continuity.
The true innovation, however, lies in the no-shave extraction protocol made possible by Choi Pen mechanics. By extracting individual follicular units through micro-punches (0.6–0.8mm diameter) without requiring donor area shaving, surgeons preserve the patient’s existing hair length to conceal extraction sites. The surrounding hair—typically 2–4cm in length for executives—masks the pinpoint scabs that form post-extraction, rendering the intervention undetectable even at conversational distance. This protocol transforms hair restoration from a visible medical event into a private biological transaction—a distinction carrying profound implications for executive adoption.
The workflow economics further favor DHI for time-constrained executives. Conventional FUE requires two distinct phases separated by 24–48 hours: extraction on day one, implantation on day two. DHI’s integrated workflow compresses both phases into a single 6–8 hour session, eliminating the logistical complexity of multi-day clinic attendance and reducing cumulative anesthesia exposure. For the executive operating on compressed calendars, this temporal compression proves decisive—enabling the entire intervention to occur within a single weekend without triggering scheduling anomalies that might alert stakeholders to medical absence.
Critically, the no-shave protocol demands superior surgical precision. Extracting follicular units through unshaved hair requires tactile discrimination to avoid transecting adjacent follicles—a skill developed only through high-volume practice. This explains why DHI outcomes show such dramatic variance between high-volume Turkish clinics (95%+ survival) and low-volume Western providers (78–85% survival). The technique’s margin for error narrows precisely where volume-driven mastery creates competitive advantage—a dynamic that has concentrated DHI excellence in Istanbul’s ecosystem of specialized clinics performing 20–30 procedures daily.
The economic implication is straightforward: executives seeking hair restoration face a binary choice. Conventional FUE requires career interruption—shaved head visibility, two-week recovery, succession speculation—or suboptimal outcomes from low-volume providers attempting no-shave techniques without requisite mastery. DHI at high-volume Istanbul clinics delivers both aesthetic superiority and operational invisibility—but only when paired with sophisticated logistical orchestration to manage the 48-hour intervention window without triggering external observation.
The Economics of Medical Arbitrage: Volume Mastery vs. Geographic Premium
The persistent misconception framing Istanbul’s hair restoration advantage as “cost arbitrage” obscures the true economic mechanism at work: volume-driven mastery creating outcome superiority unattainable in low-volume Western markets. A €15,000 FUE procedure in London does not represent premium pricing for superior quality; it reflects the economic reality of clinics performing 150–250 procedures annually attempting to amortize fixed costs (facility leases in Mayfair, regulatory compliance overhead, marketing to affluent demographics) across insufficient procedural volume. The surgeon performing three transplants weekly cannot develop the tacit knowledge—micro-adjustments for scalp tension variations, vascular mapping intuition, graft handling refinements—that emerges only through daily repetition.
Istanbul’s ecosystem operates on fundamentally different economics. Clinics like EsteNove and Hair of Istanbul perform 8,000–12,000 procedures annually across specialized teams where extraction technicians, implantation specialists, and density designers each focus on discrete workflow segments. This division of labor—unthinkable in Western clinics where single surgeons perform entire procedures—creates mastery curves impossible to replicate in low-volume environments. The technician extracting follicular units daily for three years develops tactile discrimination detecting follicle transection risk through resistance feedback—a skill no textbook can teach and no weekend course can impart. This volume-driven expertise concentrates in Istanbul not through regulatory arbitrage but through market density: Turkey’s domestic demand for hair restoration (driven by genetic predisposition and cultural emphasis on appearance) creates procedural volumes that attract global patients seeking mastery unavailable elsewhere.
The outcome differential manifests most dramatically in follicular survival rates—the ultimate metric of transplantation efficacy. Peer-reviewed studies tracking 12-month growth show Istanbul’s high-volume DHI clinics achieving 94–97% survival versus 82–88% for Western FUE providers. This 10–15 percentage point differential compounds over the five-year growth cycle into visibly superior density—particularly in the critical hairline transition zone where low survival rates create patchiness betraying transplantation. For the executive, this differential determines whether the intervention achieves aesthetic invisibility or becomes a permanent marker of medical intervention.
The pricing structure reflects this mastery concentration rather than labor cost differentials. Istanbul clinics charge €3,000–4,500 not because Turkish surgeons accept lower compensation but because high procedural volume enables cost amortization across thousands of patients rather than hundreds. The surgeon earning €250,000 annually at a high-volume Istanbul clinic achieves equivalent compensation to a London counterpart earning €450,000—but does so while performing 300 procedures annually versus 40, creating economic sustainability impossible in low-volume markets. This volume economics enables reinvestment in technology (robotic Choi Pen calibration systems, AI density mapping software) that further widens the outcome gap—a virtuous cycle inaccessible to Western clinics trapped in low-volume economics.
The executive must recognize this dynamic when evaluating providers. A London clinic charging €15,000 for “premium FUE” does not deliver superior outcomes; it delivers geographic convenience subsidized by outcome compromises necessitated by low procedural volume. The rational actor seeking optimal biological capital management accepts the logistical complexity of Istanbul travel to access volume-driven mastery—treating transportation costs not as friction but as necessary investment to access superior outcome economics. The €4,500 Istanbul procedure delivering 96% follicular survival represents superior value to the €15,000 London procedure delivering 84% survival when evaluated through the lens of aesthetic amortization over the five-year growth cycle.
This volume mastery extends beyond surgical technique to ancillary domains critical for executive adoption. Istanbul’s ecosystem has developed specialized protocols for managing post-operative edema—the forehead swelling peaking at 48–72 hours post-procedure that would trigger speculation if visible in boardroom settings. High-volume clinics deploy lymphatic drainage specialists and compression protocols reducing edema duration by 36–48 hours compared to standard care—a refinement developed through observing thousands of executive patients whose careers depend on rapid aesthetic normalization. Similarly, the no-shave protocol has been refined through iterative adjustments to extraction depth and angle based on observing how different hair textures conceal extraction sites—knowledge impossible to develop without volume.
The economic arbitrage here is not about exploiting labor differentials but about accessing mastery concentrations created by market density—a phenomenon observed across medical domains where procedural volume drives outcome superiority. Executives approaching hair restoration as biological capital management must prioritize outcome economics over geographic convenience, recognizing that the marginal cost of sophisticated travel logistics proves negligible against the career value of superior follicular survival rates.
The 48-Hour Executive Protocol: Logistics as Risk Mitigation
The DHI intervention’s theoretical elegance collapses without meticulous logistical orchestration addressing three critical vulnerability windows: pre-operative arrival visibility, post-operative transit during peak edema, and return travel before aesthetic normalization. The executive cannot afford even transient visibility of medical intervention—forehead swelling during airport transit, bandaged scalp triggering speculation among flight attendants, or visible scabbing during immigration processing could generate precisely the succession narratives the procedure aims to prevent. The 48-hour protocol succeeds only when logistics function as risk mitigation architecture rather than mere transportation.
The optimal intervention window spans Friday evening through Sunday afternoon—a temporal corridor minimizing career disruption while accommodating the 36-hour edema peak. The executive departs their home city Thursday evening on a red-eye flight, arriving Istanbul Friday morning with sufficient buffer to decompress before the 14:00 procedure start time. This pre-operative buffer proves critical: arriving fatigued increases physiological stress markers that elevate post-operative inflammation, extending edema duration. The rational actor secures premium cabin privacy not as luxury indulgence but as physiological optimization—reducing travel fatigue to minimize inflammatory response during the critical first 24 hours post-procedure.
Friday’s 14:00–21:00 procedure window aligns with circadian biology—afternoon cortisol troughs reduce inflammatory response while evening melatonin onset accelerates initial healing phases. The 7-hour DHI session concludes with immediate bandaging of donor and recipient sites, followed by a mandatory 90-minute observation period monitoring for hematoma formation. At 22:30, the executive requires transport to accommodation—but this represents the protocol’s first critical vulnerability point. Standard taxi services or ride-hailing applications introduce unacceptable risk: driver curiosity about bandaged scalp, potential photography by passengers in shared vehicles, or extended wait times exacerbating post-operative fatigue. The solution demands discreet executive transfers with three non-negotiable specifications: tinted privacy glass eliminating external visibility, direct clinic-to-accommodation routing avoiding traffic stops where bandages might be observed, and drivers trained in post-surgical patient handling (minimizing head movement during entry/exit). This ground logistics layer constitutes not convenience but risk mitigation—eliminating the single highest-probability vector for intervention visibility.
Saturday represents the edema peak phase—48 hours post-procedure when forehead swelling reaches maximum intensity. The executive must remain sequestered in accommodation with lymphatic drainage specialists performing twice-daily manual therapy to accelerate fluid reabsorption. Any external movement risks not only prolonged edema but also graft displacement during the critical anchoring phase (24–72 hours post-implantation). This sequestration requirement creates the protocol’s second vulnerability: the executive cannot order room service or receive deliveries without risking staff observation of medical intervention. The solution requires pre-arranged meal provisioning and sterile vehicle logistics for any essential external movement—such as the mandatory 18:00 clinic follow-up for bandage removal and wound assessment. The 15-minute transit to the clinic must occur in a vehicle with partitioned cabin preventing driver observation of the patient’s condition—a specification standard in medical tourism transport but absent in conventional services.
Sunday morning initiates the aesthetic normalization phase. Bandages removed at 09:00 reveal the “ugly duckling” phase—pink recipient sites and pinpoint scabs in the donor area—but crucially, the existing hair length conceals these markers from casual observation. By 12:00, gentle shampooing removes residual blood traces; by 15:00, strategic hairstyling with existing hair conceals extraction sites entirely. The executive achieves what surgeons term “social invisibility”—the capacity to move through public spaces without triggering intervention speculation—by 16:00 Sunday. This creates the narrow egress window for return travel: departing Istanbul 17:00–19:00 Sunday enables arrival at home city Monday morning with sufficient buffer before first board meeting.
This egress window introduces the protocol’s third critical vulnerability: flight delays extending transit time during the fragile 48–60 hour post-procedure window when grafts remain vulnerable to displacement. A three-hour delay at Istanbul Airport could push arrival past Monday noon—forcing the executive to attend critical meetings before achieving full social invisibility. The solution demands strategic flight contingency planning: booking return flights with 90-minute buffer windows, securing premium cabin upgrades guaranteeing priority boarding to minimize gate wait times, and arranging direct clinic-to-tarmac conveyance bypassing public airport terminals entirely through VIP services. This last specification proves decisive—executives utilizing Istanbul Airport’s MICE (Meetings, Incentives, Conferences, Exhibitions) services can transit from vehicle directly to aircraft via private jet bridge access, eliminating all public visibility during the critical egress phase.
The entire 48-hour protocol succeeds only when logistics function as integrated risk architecture rather than discrete transportation transactions. Each vulnerability window—pre-operative fatigue, post-operative edema transit, egress delay risk—requires specialized mitigation unavailable through conventional travel services. The rational actor treats logistics not as administrative overhead but as core component of biological capital management—allocating resources proportional to career risk exposure. The €300 premium for privacy-glass transfers proves negligible against the €2.5 million annual compensation at stake should intervention visibility trigger succession speculation.
Critically, this logistics architecture must be engineered pre-departure. Attempting to arrange privacy-focused transport upon arrival introduces catastrophic risk—language barriers, service unavailability during weekend hours, or driver unfamiliarity with post-surgical protocols could compromise the entire intervention’s invisibility. The executive must secure flexible medical travel booking with 24-hour modification windows to accommodate procedural timing adjustments, plus pre-vetted privacy-glass ground transport with contractual guarantees of tinted windows and partitioned cabins. This pre-engineering transforms logistics from vulnerability vector into risk mitigation layer—a distinction carrying profound implications for intervention success.
The 48-hour protocol ultimately represents not medical procedure but operational campaign requiring military-grade precision in timing, visibility management, and contingency planning. Executives approaching it as simple weekend travel invite career-compromising visibility events; those treating it as biological capital deployment engineer logistics as integral risk architecture. The difference between these approaches determines whether hair restoration extends executive tenure or accelerates its termination through poorly managed visibility.
Recovery & Social Signaling: Managing the Ugly Duckling Phase
The period between graft anchoring (72 hours post-procedure) and full aesthetic integration (9–12 months) constitutes the intervention’s most strategically complex phase—not medically, but socially. During weeks two through six, transplanted follicles enter the telogen effluvium phase: the implanted hairs shed as follicles redirect energy to establishing vascular connections, creating a temporary thinning effect that appears counterintuitive to observers unaware of transplantation biology. This “ugly duckling” phase presents the executive with a signaling dilemma: how to manage visible hair changes without triggering succession speculation during the critical period when grafts remain vulnerable to stress-induced shedding.
The optimal strategy operates through calibrated narrative management rather than concealment. Complete concealment proves impossible—close colleagues will observe subtle changes in hair texture, density patterns, and styling requirements. The executive who attempts total invisibility risks appearing evasive when questioned, triggering greater speculation than transparent management would generate. Instead, the rational actor deploys what we term “plausible deniability signaling”: acknowledging minor aesthetic adjustments without revealing medical intervention specifics. When questioned about changed appearance, the executive references “new styling techniques” or “advanced haircare regimens” developed with personal stylists—narratives sufficiently credible to satisfy casual inquiry without inviting deeper investigation.
This signaling strategy requires precise calibration. Over-communication (“I’ve started a new hair growth regimen”) invites scrutiny and follow-up questions that could unravel the plausible deniability narrative. Under-communication (“Nothing’s different”) triggers suspicion when visual evidence contradicts verbal denial. The optimal approach involves brief, matter-of-fact acknowledgment without elaboration: “Working with my stylist on density optimization” satisfies inquiry while providing no hooks for deeper investigation. This calibrated signaling maintains plausible deniability while preventing the appearance of concealment that would trigger heightened scrutiny.
The executive must also manage digital footprint during this phase. Social media posts featuring close-up photography during weeks three through five risk permanent documentation of the ugly duckling phase—images that could resurface during future leadership challenges as “evidence” of health concerns. The rational actor implements a 90-day moratorium on close-up photography in professional contexts, delegating social media content creation to communications teams trained to maintain appropriate visual distance in executive imagery. Board presentations requiring video recording should be scheduled after week six when graft shedding completes and visual normalization begins.
Workplace logistics require similar calibration. The executive should avoid situations requiring hat removal (golf outings, yacht events) during weeks two through four when scabbing remains visible under certain lighting conditions. Office climate control becomes critical—excessive heat accelerates graft shedding while dry air impedes healing. The rational actor installs personal humidifiers in office environments and avoids overheated conference rooms during the critical anchoring phase. These micro-adjustments—seemingly trivial—compound into significant outcome differentials when aggregated across the 90-day critical period.
The most sophisticated executives deploy what we term “strategic distraction signaling” during the ugly duckling phase: introducing minor, non-hair-related aesthetic adjustments that redirect observer attention from hair changes. A subtle shift in eyewear frame style, introduction of a signature accessory (pocket square, cufflinks), or minor wardrobe palette adjustment creates cognitive anchors that satisfy observers’ pattern-recognition instincts without revealing the primary intervention. The human brain seeks narrative coherence in observed changes; providing alternative explanation vectors prevents observers from fixating on hair changes as the sole variable requiring explanation.
Critically, the executive must avoid stress-induced graft shedding during this phase. Cortisol elevation from high-stakes negotiations, earnings call pressure, or board conflicts can trigger telogen effluvium in vulnerable grafts—permanently reducing final density outcomes. The rational actor implements stress mitigation protocols during weeks four through eight: delegating high-conflict negotiations, scheduling critical decisions outside this window, and deploying biofeedback techniques to maintain physiological calm during unavoidable stressors. This represents not indulgence but biological capital protection—the €3,000 procedure’s ROI depends entirely on graft survival during this fragile period.
The ugly duckling phase ultimately tests not medical outcomes but executive signaling sophistication. Those who treat it as concealment challenge invite speculation; those who deploy calibrated narrative management maintain plausible deniability while protecting graft viability through stress mitigation. The difference determines whether hair restoration extends career longevity or becomes career liability through poorly managed social optics. Biological capital management requires equal mastery of follicular science and social signaling mechanics—a dual competency separating successful interventions from counterproductive ones.
Conclusion: DHI as Biological Capital Class
The Direct Hair Implantation intervention in Istanbul’s high-volume ecosystem represents not cosmetic procedure but strategic biological capital management—a capital expenditure justified through rigorous ROI analysis when evaluated against executive career longevity economics. The €3,000–4,500 investment delivering 95%+ follicular survival rates extends productive executive tenure by 5–7 years, generating compensation and equity value multiples exceeding 2,700% ROI for typical C-suite compensation structures. This calculus transforms hair restoration from discretionary spending into fiduciary imperative for executives facing the perception-driven depreciation of the Executive Cliff.
The intervention’s viability, however, depends entirely on treating logistics as integrated risk architecture rather than administrative overhead. The 48-hour protocol succeeds only when transportation layers eliminate visibility vulnerabilities during critical edema and egress windows—requiring executive air logistics with premium cabin privacy for pre-operative fatigue mitigation, plus discreet executive transfers with tinted glass and partitioned cabins for post-operative transit. These logistics premiums—totaling €400–600—constitute not luxury indulgence but risk mitigation proportional to career exposure. The executive who treats them as optional invites precisely the visibility events that could trigger succession speculation, negating the entire intervention’s strategic purpose.
The rational actor approaches this decision through unsentimental asset management calculus. DHI represents optimal biological capital deployment for executives meeting three criteria: facing visible hairline recession triggering market perception risks; possessing schedule flexibility for 48-hour intervention window; and commanding compensation structures where 5-year tenure extension generates ROI exceeding 1,000%. For these individuals, Istanbul’s volume-driven mastery ecosystem delivers outcome superiority unattainable in low-volume Western markets—not through cost arbitrage but through procedural density creating tacit knowledge impossible to replicate elsewhere.
Conversely, the intervention proves counterproductive for executives lacking these prerequisites. Those without schedule flexibility face graft displacement risks from premature return to high-stress environments; those below €500,000 total compensation lack sufficient ROI to justify intervention costs; those with diffuse thinning patterns (rather than pattern baldness) achieve suboptimal aesthetic outcomes regardless of technique. The rational actor conducts honest self-assessment against these criteria before committing capital—recognizing that biological capital management requires matching intervention to individual depreciation curves rather than applying universal solutions.
The ultimate verdict positions DHI not as medical procedure but as strategic asset class within the executive’s human capital portfolio—a maintenance expenditure justified through NPV analysis of extended productive tenure. Its adoption signals not vanity but fiduciary sophistication: recognition that in perception-driven markets, biological appearance functions as balance sheet item requiring active management. The executive who treats hair restoration as biological capital maintenance extends career longevity through calibrated intervention; the executive who neglects it accepts accelerated depreciation through market perception mechanics entirely divorced from actual performance metrics.
Istanbul’s ecosystem has emerged as the optimal deployment venue not through regulatory arbitrage but through volume economics creating mastery concentrations unattainable elsewhere. The rational actor accepts logistical complexity to access this mastery—treating transportation costs as necessary investment to secure superior follicular survival rates. The entire intervention succeeds only when logistics function as integrated risk architecture eliminating visibility vulnerabilities during critical phases. Those who engineer this architecture transform hair restoration into seamless biological capital maintenance; those who treat it as simple medical tourism invite career-compromising visibility events.
The future of executive longevity will increasingly depend on such biological capital management strategies—not through radical life extension technologies but through calibrated interventions addressing perception-driven depreciation curves. Hair restoration represents merely the first domain where volume-driven mastery ecosystems enable outcome superiority justifying strategic capital allocation. As demographic pressures intensify succession competition, the executives who master biological capital management—treating appearance not as vanity but as fiduciary responsibility—will extend productive tenure while peers accept premature obsolescence through neglect of visible depreciation markers. In the unforgiving calculus of corporate governance, biological capital maintenance has become not optional indulgence but strategic imperative—and DHI in Istanbul’s mastery ecosystem represents its most rigorously validated deployment mechanism.